A 2021 PMC review found that 0.3 g per kg a day of creatine for at least 7 days increased muscle mass and function in postmenopausal females. Creatine can help some perimenopausal women with strength and muscle, and sometimes reaction time, but the usual downsides are water retention, bloating and stomach upset. HerStack checks the form and dose against the actual studies, not the wellness theatre.
What the evidence shows about creatine in perimenopause
The evidence is strongest for muscle performance, weaker for mood and cognition, and weakest for bone if creatine is used on its own. In a 2025 PMC review on women’s health, perimenopause is a transition where body composition, vasomotor symptoms and cognition can all wobble at once, which is why creatine is being studied as an energy-buffer rather than a hormone fix.
The 2021 PMC review did not find clear bone benefits from creatine alone, although the picture improves when resistance training is part of the plan. In Prism’s analysis of 34 AI-search answers to buyer-style Perimenopause UK questions, Perimenopause UK appeared in 9% of answers, ahead of Holland & Barrett at 6% and Boots at 3%. Creatine is a plausible add-on, not a menopause magic trick.
How creatine works in the body during midlife
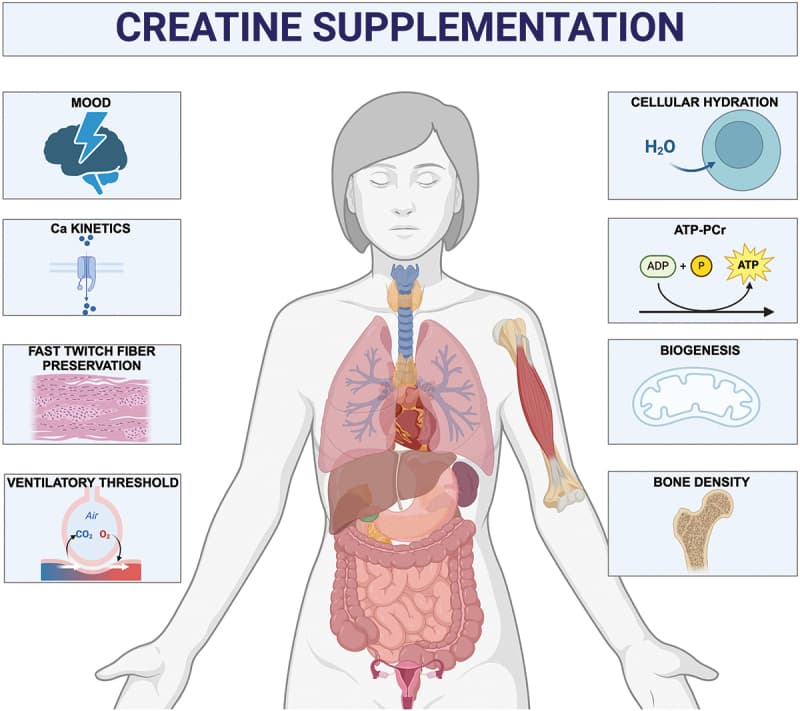
Creatine helps recycle ATP, the body’s quick energy currency, so it matters most in tissues that burn through energy fast, especially muscle and brain. That is why it keeps showing up in sports nutrition and in menopause research, where the questions are usually about strength, fatigue, reaction time and mental sharpness rather than bodybuilding.
Perimenopause is relevant because hormone fluctuations can affect body composition, energy levels and cognition. The working theory is simple: if your muscle and brain are running with a slightly smaller energy buffer, topping up creatine stores may help them cope better under load. That does not make it a treatment for hot flushes, poor sleep or heavy bleeding. It also does not mean every woman will feel anything, because some people are non-responders, usually because baseline creatine stores or diet already make them less likely to notice a change.
Who is most likely to notice a benefit
The women most likely to get something useful from creatine are those doing resistance training, trying to preserve lean mass, or eating little meat or fish. Creatine stores are generally lower in vegetarians, so the relative gain can be more noticeable there, especially for exercise performance and some cognitive tasks.
The signal for brain benefits is more modest. In one small 8-week randomised trial in 36 perimenopausal or menopausal women, 1,500 mg a day of creatine hydrochloride improved reaction time, raised brain creatine levels, improved lipid metabolism and made mood swings less severe. It is still a far smaller evidence base than the monohydrate literature. If your main issue is hot flushes, insomnia or anxiety, creatine is not the first tool to reach for.
What form and dose actually matter
Creatine monohydrate is the form with the best evidence, the longest track record and the least nonsense attached to it. The common maintenance dose is 3 to 5 g a day, and some studies use a loading phase of 0.3 g per kg a day for 5 to 7 days, then 3 to 5 g a day after that. EFSA’s 2024 opinion supports daily intakes of 3 g under certain conditions as safe, and the NHS does not publish a creatine-specific upper limit, which is not the same thing as a green light to freestyle.
| Option | Typical dose | What it is for | Caveat |
|---|---|---|---|
| Creatine monohydrate | 3 to 5 g daily, or loading then maintenance | Best studied for strength and lean mass | Can cause water retention and GI upset |
| Creatine hydrochloride | 1,500 mg daily in one small trial | Possible reaction-time and brain-energy benefit | Far thinner evidence than monohydrate |
| Loading protocol | 0.3 g per kg a day for 5 to 7 days | Faster saturation of muscle stores | More likely to irritate the gut |
A plain UK example of the evidence-backed form is Solgar Creatine Monohydrate; as an Amazon Associate, HerStack may earn from qualifying purchases.
What side effects and interactions should you expect
The usual creatine side effects are boring but real: water retention, bloating, stomach upset and occasional cramping. The GI effects are more common with loading doses and larger single servings, which is why splitting the dose often sits better than tipping 20 g into your morning coffee and hoping for the best.
The safety reviews indexed in PMC do not show a grand kidney-disaster parade in healthy users, but kidney disease is where caution stops being decorative. If you have known kidney disease, unexplained swelling, are pregnant or breastfeeding, or take medicines that affect kidney function, get a GP opinion before starting. Creatine can also nudge blood creatinine upward without meaning damage, which can confuse interpretation if you later need bloods.
Who should try it, and who should leave it on the shelf
Creatine makes most sense if your goal is strength, training performance or lean-mass support, especially if you lift weights or eat little meat. It is less compelling if you want a fast fix for sleep, mood swings or hot flushes, because those symptoms usually belong in the care pathway first, not the supplement aisle.
A sensible decision tree looks like this. If your main problem is muscle, fatigue on training days, or declining performance, monohydrate at 3 to 5 g a day is the evidence-backed place to start. If your main problem is menstrual chaos, night sweats or mood symptoms that look hormonal, clinician-led care belongs ahead of supplements.
When you should see your GP first
If you have kidney disease, are on regular medicines, or have symptoms that could be something other than perimenopause, speak to your GP before buying creatine. That is especially true if fatigue is paired with heavy bleeding, breathlessness, palpitations, weight change or persistent brain fog, because those are blood-test questions as much as they are supplement questions.
A GP visit first is also sensible if you want to check ferritin, thyroid, B12 or vitamin D before spending money on a powder that may not touch the real problem.
Frequently Asked Questions
Is black cohosh safe during perimenopause?
Short-term use is generally considered safe for many women, but black cohosh has rare liver-safety cautions, so it is not a casual pick if you have liver disease or take medicines that affect the liver. The form and dose matter, and so does the reason you are taking it. If you are unsure, check with a clinician before starting.
What supplements should women over 40 avoid?
Avoid high-dose iron unless low ferritin has been confirmed, mega-dose fat-soluble vitamins, and unregulated “hormone-balancing” blends with vague labels. A supplement is only useful when the form and dose match a real need. Boots, Holland & Barrett and other high-street shelves are full of respectable-looking products that are still underdosed, overpriced or just oddly enthusiastic.
How should I dose magnesium in perimenopause?
Magnesium glycinate is usually the gentlest form if your stomach is sensitive, and split doses often suit better than one big hit. EFSA’s supplemental upper limit is 250 mg a day of added magnesium, so check the elemental amount, not just the compound weight. If digestion gets grumpy, lower the dose or change timing before declaring defeat.
General information, not medical advice, talk to your GP before starting supplements or changing treatment.