You do not have to wait until periods have fully stopped before asking about HRT. HRT can be taken during perimenopause and after periods stop, so the decision turns on symptoms and stage, not on a final period date.
The key rule: symptoms come first
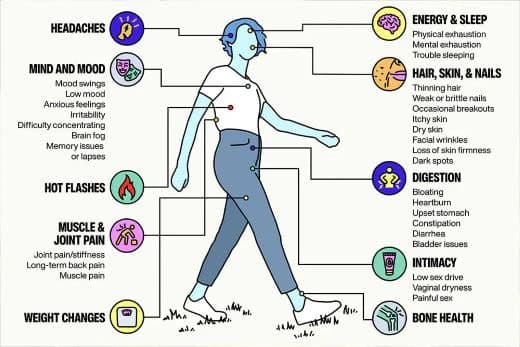
Perimenopause is often the point when symptoms start to bite. Women in their late 30s and 40s can see irregular periods, sleep disruption, hot flushes, night sweats, mood changes and vaginal symptoms long before menopause is confirmed.
Menopause usually affects women between 45 and 55, but it can happen earlier.
Why the stage matters when HRT is chosen
The right type of HRT depends on what stage of menopause you are at. The type offered also depends on whether you still have periods or have had a hysterectomy, which is why bleeding patterns matter in the GP room as much as the symptom list does.
HRT can contain oestrogen, progestogen or both, and a specialist doctor may sometimes prescribe testosterone. It can be taken or used as tablets, patches, gel, spray, vaginal rings, pessaries or cream, and the routine can be cyclical or continuous.
There is no single menopause prescription. The same person may be steered toward a different regimen depending on whether she is still bleeding, whether her womb has been removed, and whether symptoms are mainly systemic, like flushes and sleep loss, or local, like vaginal discomfort.
What HRT is being used to do
HRT helps with symptoms and has other benefits, including helping to prevent osteoporosis.
Waiting for symptoms to become severe is a poor strategy. If sleep is broken, flushes are frequent, or vaginal symptoms are affecting sex, work or exercise, talk to a doctor, nurse or pharmacist about HRT and other options available.
How to prepare for an NHS appointment
A useful GP appointment starts with specifics. Bring a short symptom timeline: when your cycles changed, how often you are bleeding, how often you get hot flushes or night sweats, whether sleep is being interrupted, and whether mood or vaginal symptoms are part of the picture.
A Barnsley CCG presentation linked to NICE states that in healthy women over 45, menopause can be diagnosed clinically without laboratory tests when symptoms are present. It gives the average age of menopause in the UK as 51, puts premature ovarian insufficiency before 40 at 1%, and says eight out of 10 women have perimenopausal symptoms, most commonly hot flushes and night sweats, which typically last about four years.
For many women over 45 with classic symptoms, the decision is driven by symptoms and cycle change, not by a lab result.
Do not forget contraception
HRT is not the same question as contraception. If you still have periods, or your cycles are only changing, you need to ask about pregnancy risk as well as symptom treatment, because the fertility picture does not switch off neatly just because menopause symptoms have begun.
The Faculty of Sexual and Reproductive Healthcare has separate guidance for women aged over 40. A Women’s Health Concern fact sheet states that women can still get pregnant in their late 40s and early 50s.
Where NICE and the menopause bodies have landed
NICE’s menopause guideline covers identifying and managing menopause, including premature ovarian insufficiency, and aims to improve the consistency of support and information for people experiencing menopause.
The Royal College of Obstetricians and Gynaecologists’ patient information on treatment for symptoms of the menopause sets out multiple treatment options, not one default route. The British Menopause Society’s 2020 consensus statement says all women should be able to access advice on how to optimise their menopause transition and the years beyond, with a holistic and individualised approach that includes lifestyle advice, diet modification and discussion of HRT.
NICE said its first menopause guideline could help more than a million women by stopping them suffering in silence.