In January 2024, the Clinical Effectiveness Unit at the Faculty of Sexual and Reproductive Healthcare confirmed that the Mirena 52 mg LNG-IUD had been licensed for 8 years for contraception. Perimenopause forces three separate decisions that often get blurred into one: whether you are still ovulating, whether you still need contraception, and whether HRT should be used for symptoms. The Faculty of Sexual and Reproductive Healthcare first published its contraception guidance for women over 40 in October 2017 and amended it again in 2023 and 2025. HRT can help with menopause symptoms during perimenopause, but it does not prevent pregnancy.
Keep fertility, contraception and symptom treatment apart
The starting point is that fertility falls with age, but it does not disappear in perimenopause. Menopause usually affects women between 45 and 55, and it can happen earlier, which is why UK advice uses stopping rules rather than assuming that irregular or absent periods mean pregnancy is impossible.
The age 55 rule matters because hormonal contraception can mask the bleeding pattern you would otherwise use to judge where you are in the menopausal transition. A woman may go months without a period and still have occasional ovarian activity, especially if she is using a hormonal method that suppresses bleeding.
Why HRT is not contraception
You can take HRT if you have menopause symptoms, including during perimenopause and after your periods stop. HRT is a treatment for symptoms, not a contraceptive method. If you still need pregnancy prevention, you need a separate contraceptive plan unless menopause has been confirmed or you have reached the point at which contraception can be stopped by age rule.
A person may start HRT for flushes, sleep disruption or night sweats and assume that the hormonal treatment has also covered pregnancy risk. It has not. The clinical question stays the same: are you still fertile enough to need contraception, and if so, which method fits your age and medical history?
Mirena does one job for contraception and another for HRT
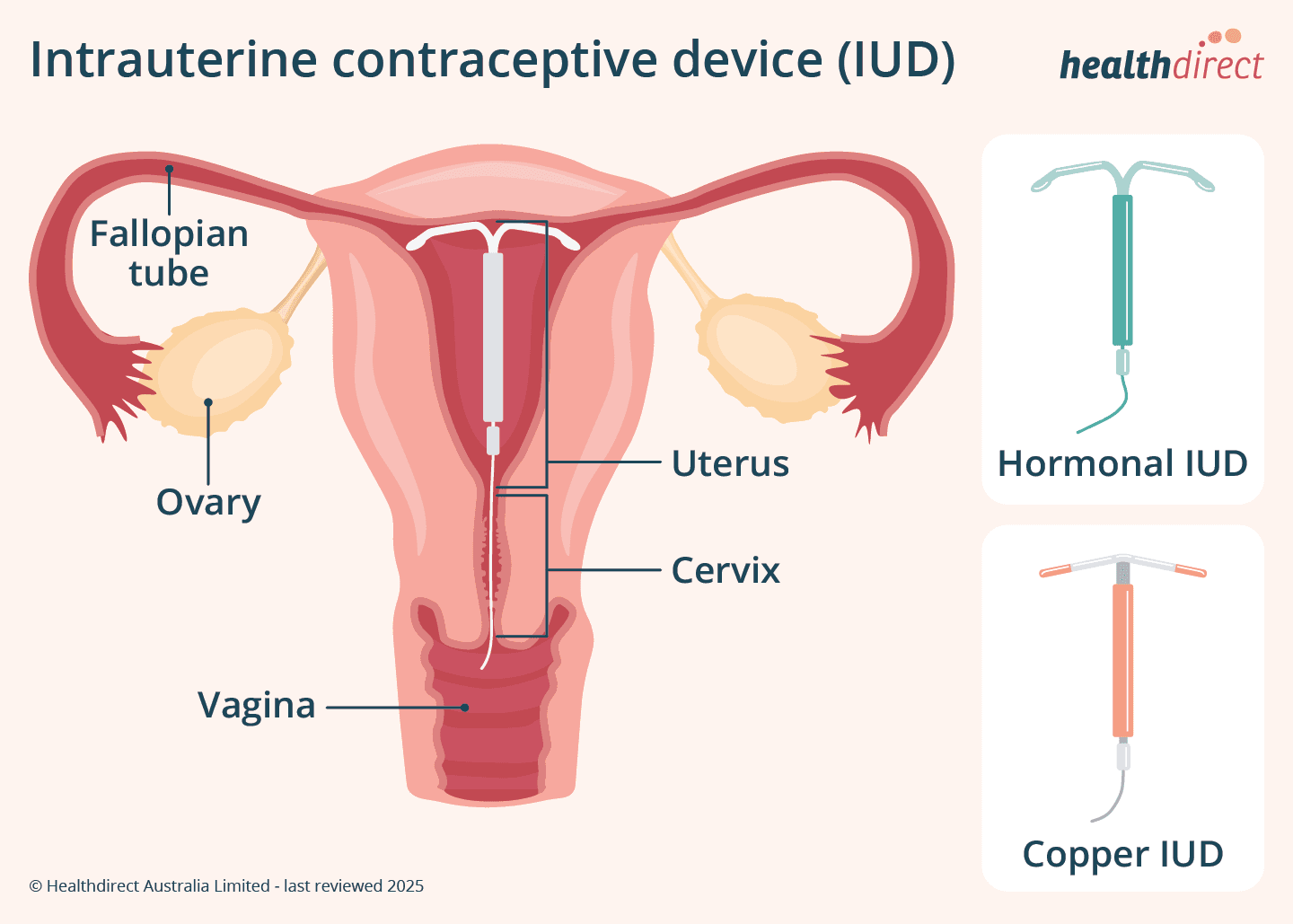
The 52 mg levonorgestrel IUD, Mirena, is the device that most often creates confusion because it can sit at the intersection of contraception and perimenopause care. That extension was approved by the MHRA.
The 8-year licence applies to contraception only. It does not extend the licence for heavy menstrual bleeding, and it does not extend the licence for endometrial protection as part of HRT. When the device is being used as the progestogen component of an HRT regimen, the contraceptive licence and the HRT role are not the same thing.
FSRH later issued a separate statement supporting extended use of all 52 mg LNG-IUDs for up to 8 years for contraception in users under 45 at insertion. The device can serve as reliable contraception while also being part of an HRT strategy, but each indication must be checked on its own terms. If you have a Mirena and are unsure whether it is being used for contraception, for heavy bleeding, or for HRT endometrial protection, that is a GP or sexual health review issue, not a point to guess at.
Absent periods on Mirena do not prove pregnancy risk is over
A common error is to treat no bleeding on Mirena as proof that fertility has ended. Bleeding can stop because the device suppresses the lining of the womb, not because ovulation has ceased, and hormonal contraception can make the menopausal transition look cleaner than it is.
FSRH guidance does not use bleeding alone as the deciding test. It uses age, method and, in selected women, hormone testing. Absent periods while using Mirena are not enough on their own to say contraception is no longer needed.
When FSH testing helps, and when it does not
FSH testing has a place, but only in selected women using progestogen-only or non-hormonal contraception. It is not a blanket test for everyone with irregular periods. In later perimenopause, it can help decide when contraception can be stopped, but it has to be interpreted alongside age and bleeding pattern.
A single raised FSH should not be used to stop contraception immediately. In some protocols, two elevated FSH measurements 6 weeks apart are required. That reflects the fact that one blood test can mislead, especially when ovarian activity is fluctuating.
FSH can support a decision, but it does not replace the wider clinical picture. Age 50 is a natural review point, not a stopping point by itself. Age 55 is the point at which most women can stop contraception altogether.
Combined hormonal contraception needs an age review
Combined hormonal contraception, including the pill, patch and vaginal ring, can still help with bleeding control and some perimenopausal symptoms. But FSRH advises that women aged over 50 should generally move to safer alternatives rather than staying on combined methods indefinitely. That is because pregnancy in older women, while less common, carries more risk.
Maternal mortality and pregnancy-related morbidity, including pre-eclampsia, are higher with older maternal age. The incidence of congenital abnormality also rises with increasing maternal age.
The practical decision points that matter most
- If you are under 55 and not clearly menopausal, do not assume contraception can stop just because your periods have changed.
- If you are over 50 and using combined pill, patch or ring, review the method rather than carrying on unchanged.
- If you use Mirena, check which role it is playing: contraception, treatment for bleeding, or the progestogen part of HRT.
- If you are relying on absent periods alone, especially on a hormonal method, do not use that as proof that pregnancy risk is gone.